










Cannabis and genetics: why we don't all react the same way
- sensculture

- 6 days ago
- 3 min read

One of the most common mistakes when discussing cannabis is assuming its effects are universal, when in clinical practice the exact opposite is true: two people can consume the same dose, of the same product, and by the same route, and experience radically different effects. This variability is not anecdotal or psychological; it has a solid biological basis, and a significant part of it is genetic.
Today, thanks to direct-to-consumer genotyping tests like those from 23andMe, it's possible to access information that was previously only available in research settings. However, the real value lies not in taking the test, but in knowing what to look for within the raw data and how to interpret it with clinical judgment and common sense.
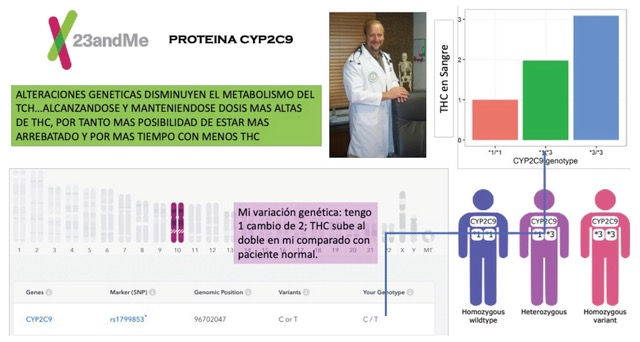
Cannabis, particularly THC, doesn't act solely based on the dose consumed, but also on how long it remains active in the body. This is where liver enzymes of the cytochrome P450 system come into play, especially CYP2C9, which is responsible for metabolizing a significant portion of THC. Common genetic variants such as CYP2C9 2 and CYP2C9 3 reduce this metabolic capacity, resulting in higher plasma concentrations, more intense and prolonged effects, and a greater likelihood of anxiety, dysphoria, or a subjective experience of being "too high" with doses that would be moderate for others.
The graph presented illustrates precisely this phenomenon using a real-world example: my own genetic profile as a patient. In my case, a variant in CYP2C9 identified in the raw data from 23andMe shows a reduced capacity to metabolize THC. In practical terms, this means that, compared to a person without this variation, the same dose of THC can double its blood level and remain active for a longer period. This information objectively explains why some people, including myself, require lower doses and greater spacing between doses to achieve the same therapeutic effect without adverse effects. This is not about tolerance, suggestion, or emotional fragility; it is about applied pharmacogenetics.
Many patients who describe themselves as “highly sensitive” to cannabis fit this profile. This information is often present in the raw data from genetic testing, although it is not always clearly presented in standard commercial reports. Analyzing this data with external genetic interpretation tools can contextualize individual experiences and help avoid common dosing errors.
Another layer of variability occurs at the level of the central nervous system, particularly in the type 1 cannabinoid receptors, encoded by the CNR1 gene. Certain variants are associated with greater sensitivity to the psychoactive effects of THC, while others appear to dampen them. This explains why some people experience intense perceptual changes with low doses, while others feel little effect even with higher amounts.
In addition, cannabis indirectly interacts with the dopaminergic system. Genes such as COMT, especially the Val158Met polymorphism, modulate dopamine availability in the prefrontal cortex and can influence the emotional and cognitive response to THC. This does not mean that a person is "destined" to develop psychosis, but it does mean that, in combination with high doses, frequent use, high-potency products, or early initiation, the impact can vary depending on the genetic profile.
Other genes, such as AKT1 and DRD2, as well as components of the extended endocannabinoid system, or endocannabinodome, also contribute to this diversity of responses, influencing stress management, memory, attention, and emotional regulation. This is why two people can use cannabis for the same therapeutic purpose and obtain very different results.
The practical process for accessing this information involves downloading the raw genetic profile data, analyzing it on specialized platforms, and, above all, interpreting it within a prudent and non-alarmist clinical framework. Genetics is not a diagnosis or a sentence; it is a contextual tool that allows us to anticipate responses, adjust dosages, and reduce avoidable risks.
When this information is integrated into clinical practice, the focus shifts from a binary discourse of "consume or don't consume" to one of personalized medicine: starting with low doses, increasing slowly, spacing out doses, prioritizing CBD formulations, avoiding high THC in slow metabolizers, and observing the actual individual response rather than comparing oneself to the experience of others.
Cannabis doesn't act in a vacuum. It acts on a unique organism, with a particular history, context, and biology. Accessing genetic information is possible today; interpreting it sensibly and applying it prudently is what transforms that knowledge into a clinical tool for safer, more precise, and truly conscious use.

Dr. Jaime Claudio Villamil
Professor of Cannabis Medicine, Clinician and Researcher, education, dosage and risk reduction in cannabis et al.

Comments